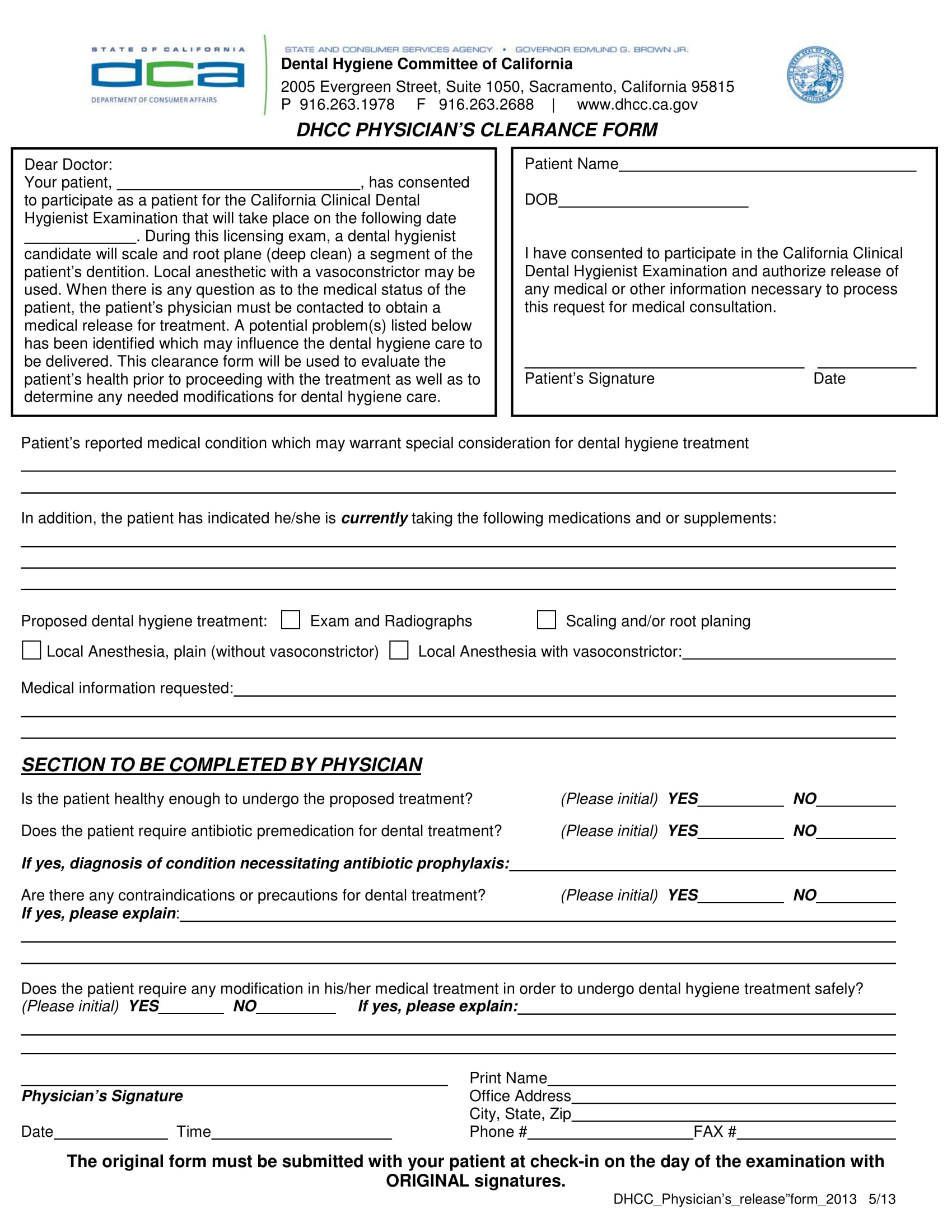
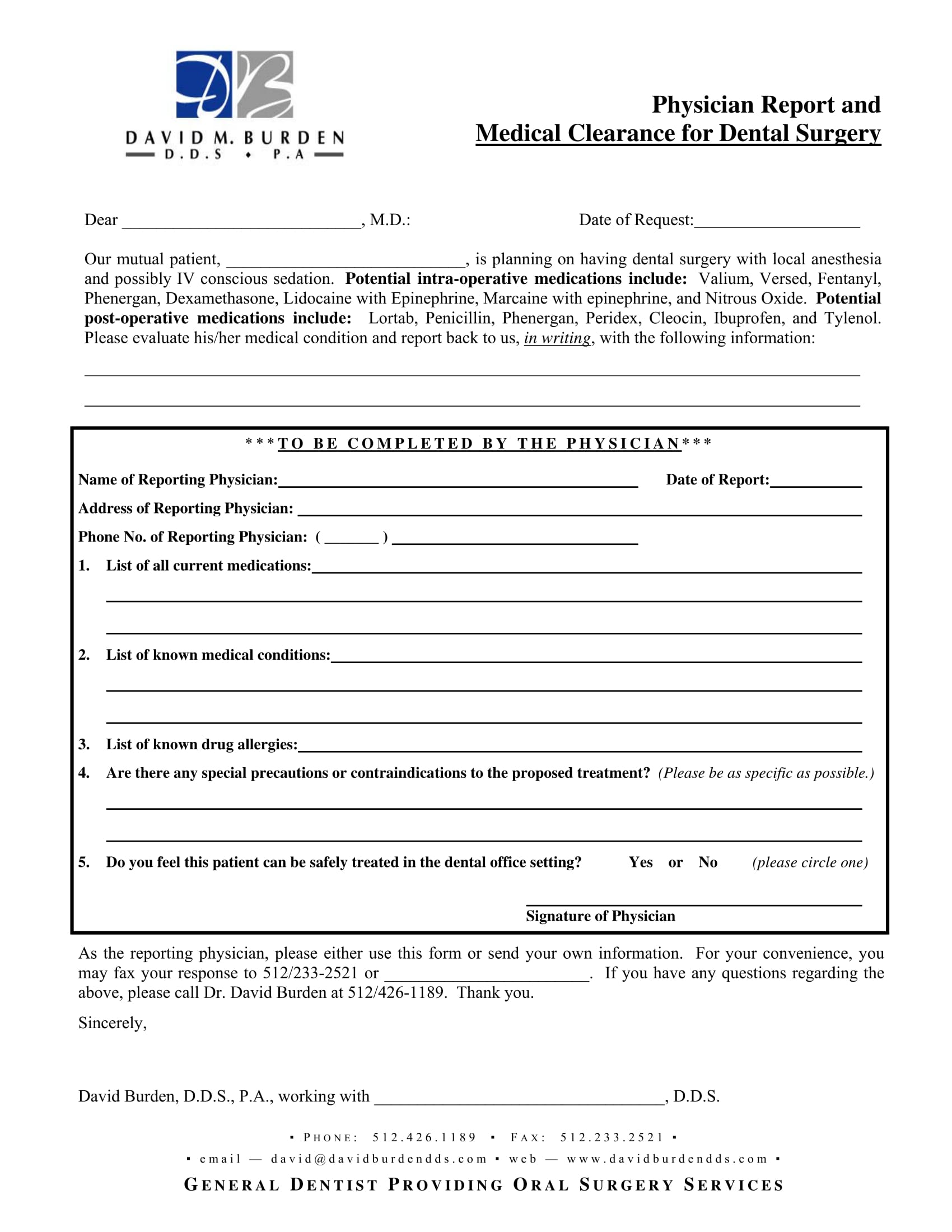
Printable Medical Clearance Form For Dental Treatment – Medical clearance form (confidential) referring doctor: Paperless solutionspaperless workflowfree mobile appedit on any device Your patient (listed above) is being scheduled for dental procedures that may require the administration of general anesthesia or iv sedation. Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical exam:_____________ dear physician: Our mutual patient, as noted above, is scheduled for dental treatment at our office. Our mutual patient, as noted above, is scheduled for dental treatment at our office. Please review the reasons checked below. Cleaning (simple or deep) root canal therapy. Physician report and medical clearance for dental surgery. This article presents recommendations related to patients with certain medical conditions who are planning to undergo common dental procedures, such as cleanings, extractions, restorations,.
Printable Dental Clearance Form For Surgery
We have enclosed a form that may save you time. Is the patient an acceptable candidate for. Our mutual patient, as noted above, is scheduled for dental treatment at our office. ____________________________________ our mutual patient, _____________________________________________________ is scheduled for dental. Medical clearance for dental treatment.
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
Our mutual patient, as noted above, is scheduled for dental treatment at our office. Medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical exam:_____________ dear physician: This article presents recommendations related to patients with certain medical conditions who are planning to undergo common dental procedures, such as cleanings, extractions, restorations,. Is the patient an acceptable candidate for..
Printable Medical Clearance Form For Surgery Printable Word Searches
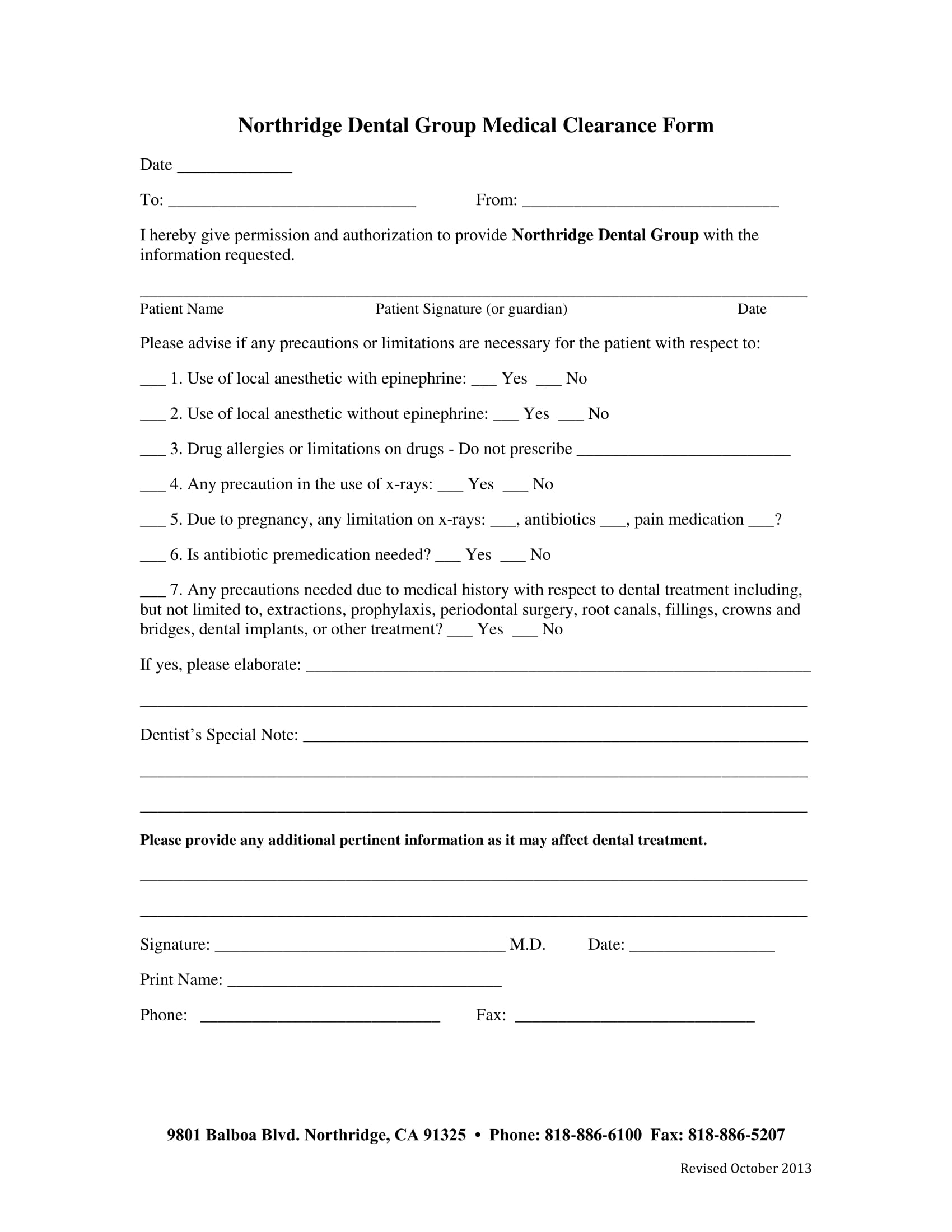
Cleaning (simple or deep) root canal therapy. I hereby authorize the dental team to perform the necessary dental procedures as discussed and agreed upon. We have enclosed a form that may save you time. Medical clearance for dental treatment. If you’re a dental office manager, use a free dental clearance form template to collect patient information online!
Printable Medical Clearance Form For Dental Treatment
Up to $32 cash back complete medical clearance form for dental online with us legal forms. ____________________________________ our mutual patient, _____________________________________________________ is scheduled for dental. Physician report and medical clearance for dental surgery. Our mutual patient, as noted above, is scheduled for dental treatment at our office. Cleaning (simple or deep) root canal therapy.
FREE 29+ Sample Medical Clearance Forms in PDF Word Excel
Paperless solutionspaperless workflowfree mobile appedit on any device Our mutual patient, as noted above, is scheduled for dental treatment at our office. Your patient (listed above) is being scheduled for dental procedures that may require the administration of general anesthesia or iv sedation. If you’re a dental office manager, use a free dental clearance form template to collect patient information.
Our Mutual Patient, As Noted Above, Is Scheduled For Dental Treatment At Our Office.
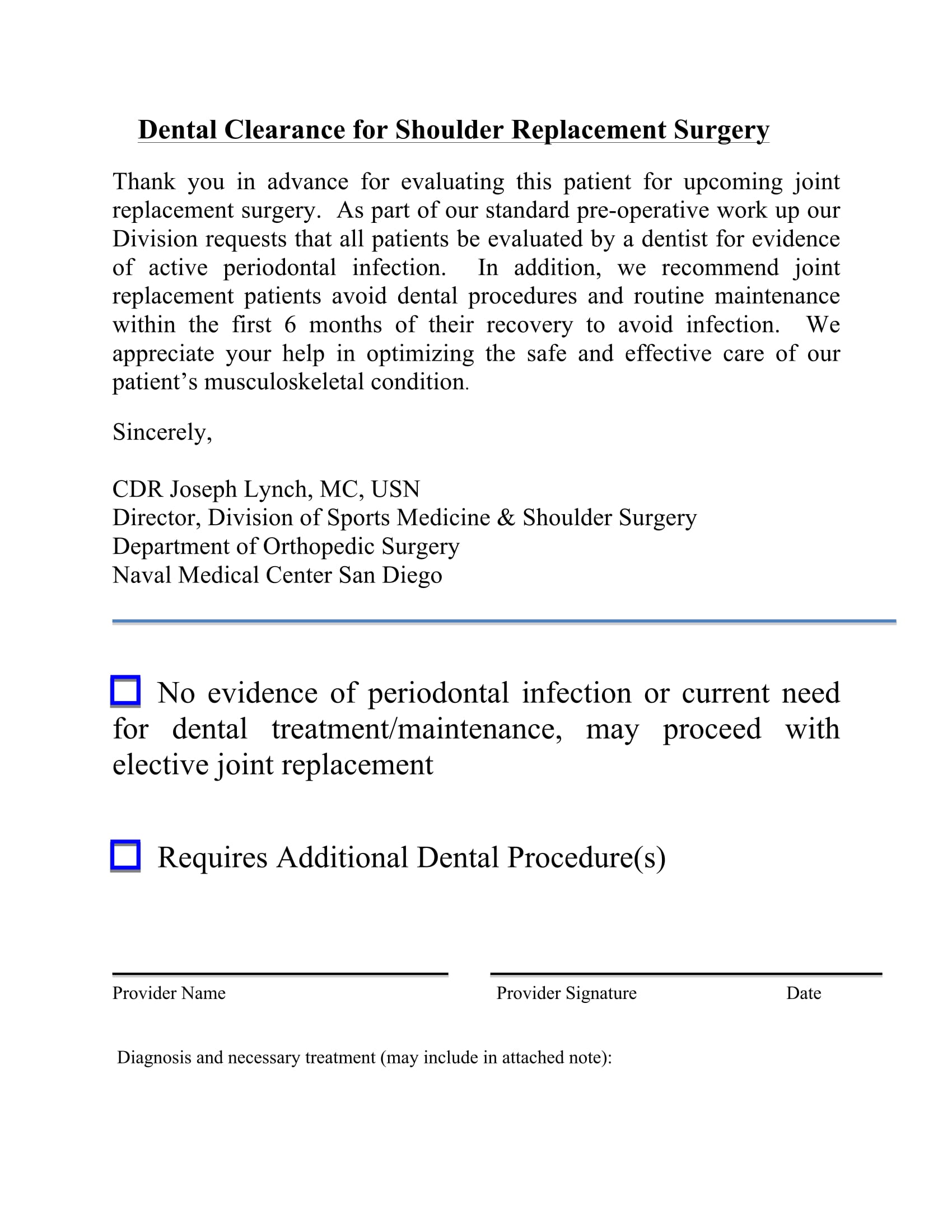
This article presents recommendations related to patients with certain medical conditions who are planning to undergo common dental procedures, such as cleanings, extractions, restorations,. Medical clearance for dental treatment. Our mutual patient, as noted above, is scheduled for dental treatment at our office. Please review the reasons checked below.
Paperless Solutionspaperless Workflowfree Mobile Appedit On Any Device
Your patient (listed above) is being scheduled for dental procedures that may require the administration of general anesthesia or iv sedation. ____________________________________ our mutual patient, _____________________________________________________ is scheduled for dental. I understand that during the course of treatment, unforeseen conditions may Our mutual patient, as noted above, is scheduled for dental treatment at our office.
Medical Clearance For Dental Treatment Patient’s Name:_________________________ D.o.b:______________ Date Of Last Physical Exam:_____________ Dear Physician:
If you’re a dental office manager, use a free dental clearance form template to collect patient information online! Easily fill out pdf blank, edit, and sign them. Cleaning (simple or deep) root canal therapy. Save or instantly send your ready.
We Have Enclosed A Form That May Save You Time.
Just customize the form to match your dental office’s look and feel — then. I hereby authorize the dental team to perform the necessary dental procedures as discussed and agreed upon. In an attempt to provide the best and safest dental care for this patient, we are requesting medical consultation and authorization. Up to $32 cash back complete medical clearance form for dental online with us legal forms.